 First Degree AV Block ECG Example
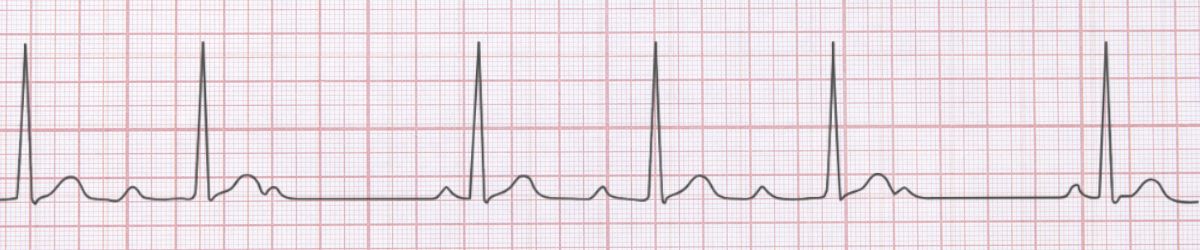
Figure 1: First Degree AV Block - Characteristic ECG Pattern
First Degree AV Block ECG Example
Figure 1: First Degree AV Block - Characteristic ECG Pattern
🔑 Key Points at a Glance
- Heart Rate: Normal sinus rate (60-100 bpm)
- Primary Significance: Usually benign, may indicate AV nodal disease, can progress to higher degrees
- Key Management: Monitor for progression, identify reversible causes (medications, ischemia)
- Clinical Category: Education
Overview and Clinical Significance
First Degree AV Block represents an important cardiac rhythm pattern that clinicians must accurately identify. Usually benign, may indicate AV nodal disease, can progress to higher degrees
Understanding this rhythm is essential for emergency physicians, cardiologists, intensivists, and all healthcare providers involved in acute cardiac care. Early recognition and appropriate management can significantly impact patient outcomes.
ECG Characteristics and Recognition
📊 Diagnostic ECG Criteria
- PR interval >0.20 seconds
- Every P wave conducted
- 1:1 AV conduction
- Regular rhythm
Systematic ECG Analysis Approach
When analyzing any ECG, including suspected First Degree AV Block, follow this systematic approach:
- Rate: Calculate the ventricular rate using the 300-150-100-75-60-50 rule or count complexes in 6 seconds × 10
- Rhythm: Assess regularity by measuring R-R intervals across the strip
- P Waves: Identify presence, morphology, and relationship to QRS complexes
- PR Interval: Measure from start of P wave to start of QRS (normal: 0.12-0.20 seconds)
- QRS Complex: Assess duration (normal: 1mm is significant)
- T Waves: Check morphology, direction, and concordance with QRS
- QT Interval: Measure and correct for heart rate (QTc normal: Most patients with this rhythm are asymptomatic - focus on patient education and appropriate reassurance
Evidence-Based Management
Acute Management Strategy
Primary Treatment Approach: Monitor for progression, identify reversible causes (medications, ischemia)
Pharmacologic Interventions
Most cases require no pharmacologic intervention - focus on treating underlying causes and monitoring for progression.
Procedural Considerations
Procedural intervention is rarely required - conservative management is typically appropriate.
Differential Diagnosis
🔍 Consider These Mimics
- Normal PR interval in presence of LVH or cardiomegaly
- Measurement error - ensure proper lead placement
Complications and Risk Stratification
Potential complications associated with First Degree AV Block include:
- Progression to more severe conduction abnormalities
- Symptoms interfering with quality of life
Long-Term Management and Follow-Up
Routine follow-up is generally not required unless symptoms develop or underlying cardiac disease is identified.
📅 Follow-Up Recommendations
- Primary care follow-up as needed
- Reassurance and education regarding benign nature
- Lifestyle modifications: exercise, stress reduction, avoid triggers
Common Pitfalls and How to Avoid Them
⚠️ Common Mistakes to Avoid
- Failing to correlate ECG with clinical presentation
- Missing underlying reversible causes
- Not consulting cardiology when uncertain
Patient Education and Counseling
When counseling patients diagnosed with First Degree AV Block, address the following key points:
- Nature of the condition: Explain the rhythm abnormality in simple terms, avoiding medical jargon
- Prognosis: Reassure about the benign nature and excellent prognosis
- Warning signs: Educate about symptoms requiring immediate medical attention (chest pain, syncope, severe dyspnea)
- Medication compliance: Typically no medications required
- Lifestyle modifications: Limit caffeine and alcohol, maintain healthy weight, exercise regularly (as tolerated), stress reduction
- Activity restrictions: No activity restrictions - encourage normal physical activity
Evidence-Based Guidelines and References
Current management of First Degree AV Block is based on evidence from major clinical trials and consensus guidelines from professional societies including:
- American Heart Association (AHA) / American College of Cardiology (ACC) Guidelines
- European Society of Cardiology (ESC) Guidelines
- Advanced Cardiac Life Support (ACLS) Protocols
- Heart Rhythm Society (HRS) Expert Consensus Statements
📚 Level of Evidence
Most recommendations for acute management of First Degree AV Block are supported by Level C (expert consensus and observational data) evidence.
Summary and Clinical Bottom Line
📋 Clinical Bottom Line
First Degree AV Block is characterized by pr interval >0.20 seconds and every p wave conducted. Usually benign, may indicate AV nodal disease, can progress to higher degrees Management priority: Monitor for progression, identify reversible causes (medications, ischemia) Key takeaway: Recognition and reassurance are the primary interventions needed
About the Author
Dr. Raj K
Emergency Medicine Physician Dr. Raj K is a board-certified Emergency Medicine physician with extensive experience in acute cardiac care and ECG interpretation. He is passionate about medical education and bringing evidence-based emergency medicine knowledge to healthcare providers worldwide through E-PulsePoints.