 Right Bundle Branch Block (RBBB) ECG Example
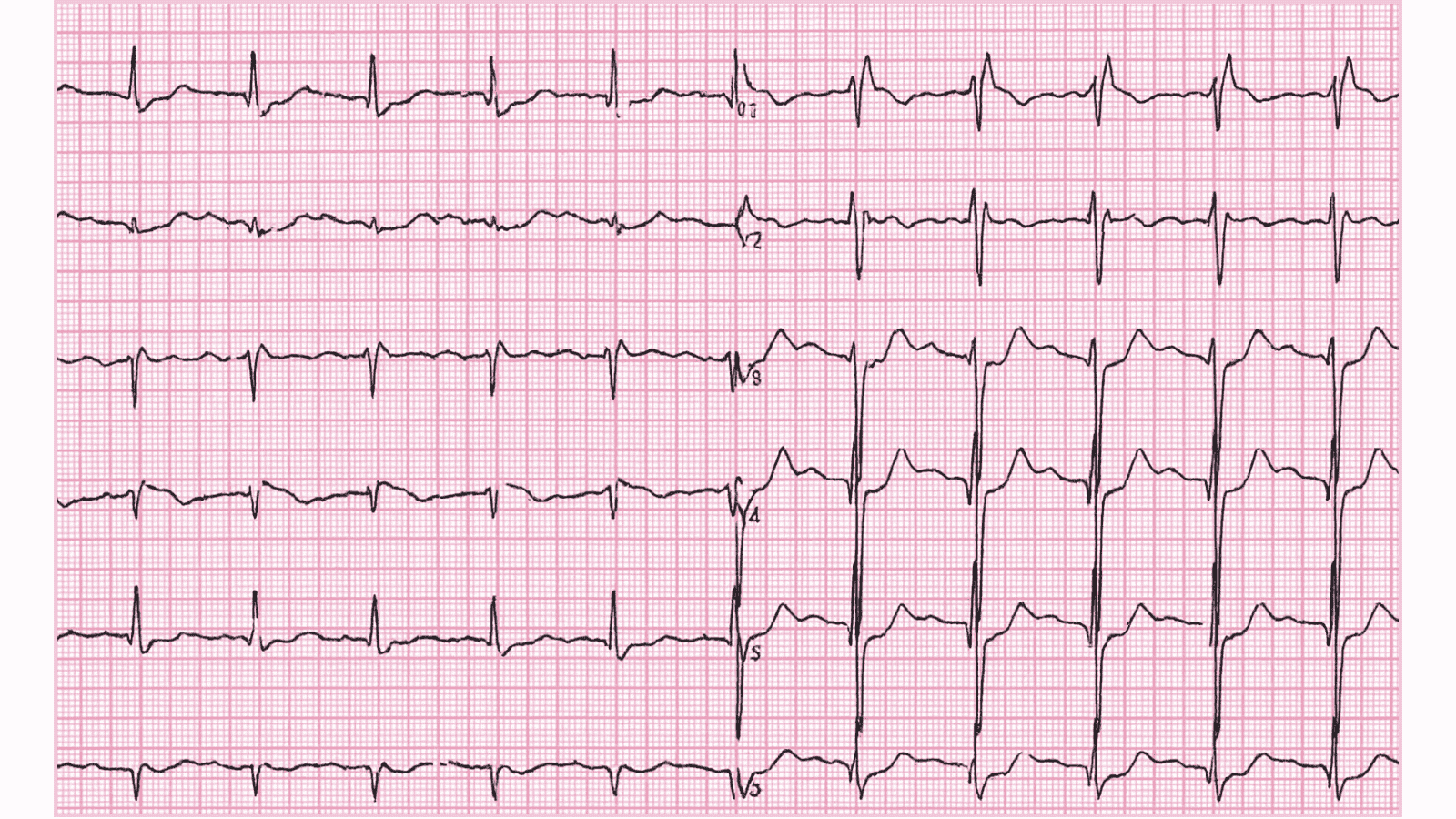
Figure 1: Right Bundle Branch Block (RBBB) - Characteristic ECG Pattern
Right Bundle Branch Block (RBBB) ECG Example
Figure 1: Right Bundle Branch Block (RBBB) - Characteristic ECG Pattern
🔑 Key Points at a Glance
- Heart Rate: Variable, underlying rhythm determines rate
- Primary Significance: May be normal variant or indicate RV strain/pathology, ischemia still interpretable unlike LBBB
- Key Management: Investigate for underlying cause if new, evaluate for pulmonary embolism if acute onset, usually no specific treatment
- Clinical Category: Education
Overview and Clinical Significance
Right Bundle Branch Block (RBBB) represents an important cardiac rhythm pattern that clinicians must accurately identify. May be normal variant or indicate RV strain/pathology, ischemia still interpretable unlike LBBB
Understanding this ECG finding is essential for emergency physicians, cardiologists, intensivists, and all healthcare providers involved in acute cardiac care. Early recognition and appropriate management can significantly impact patient outcomes and prevent life-threatening complications.
ECG Characteristics and Recognition
📊 Diagnostic ECG Criteria
- QRS >120ms (wide)
- RSR' pattern in V1-V2 (M-shaped)
- Wide slurred S wave in I, V5-V6
- ST depression and T wave inversion in V1-V2
Systematic ECG Analysis Approach
When analyzing any ECG, including suspected Right Bundle Branch Block (RBBB), follow this systematic approach:
- Rate: Calculate ventricular rate using the 300-150-100-75-60-50 rule or count QRS complexes in 6 seconds × 10
- Rhythm: Assess regularity by measuring R-R intervals across the entire strip
- P Waves: Identify presence, morphology, and relationship to QRS complexes
- PR Interval: Measure from start of P wave to start of QRS (normal: 0.12-0.20 seconds or 3-5 small squares)
- QRS Complex: Assess duration (normal: Correlate ECG findings with clinical presentation - the patient at the bedside determines urgency, not just the ECG pattern
Evidence-Based Management
Acute Management Strategy
Primary Treatment Approach: Investigate for underlying cause if new, evaluate for pulmonary embolism if acute onset, usually no specific treatment
Stepwise Treatment Algorithm
Step 1: Initial Stabilization
- Ensure hemodynamic stability - check blood pressure, perfusion, mental status
- Obtain IV access and send labs (troponin, BMP, CBC, coags, BNP if heart failure suspected)
- Continuous telemetry monitoring in appropriate care setting
- Serial ECGs to assess for dynamic changes
Step 2: Definitive Management
Investigate for underlying cause if new, evaluate for pulmonary embolism if acute onset, usually no specific treatment
Pharmacologic Interventions
Most cases require no specific pharmacologic intervention - focus on treating underlying causes and monitoring for progression.
Differential Diagnosis and ECG Mimics
🔍 Consider These Alternative Diagnoses
- Similar ECG patterns to distinguish from: Careful analysis of specific ECG criteria, clinical context, and patient presentation is essential for accurate diagnosis
- Use systematic approach: Compare rate, rhythm, P wave morphology, PR interval, QRS width, and ST-T changes
- When in doubt: Obtain cardiology consultation, compare to old ECGs, correlate with clinical presentation
Complications and Risk Stratification
Potential complications and adverse outcomes associated with Right Bundle Branch Block (RBBB):
- Immediate risks: Progression to more severe arrhythmia, syncope, hemodynamic compromise
- Short-term complications: Syncope, pre-syncope, fatigue, reduced exercise tolerance
- Long-term sequelae: Tachycardia-induced cardiomyopathy if persistent, quality of life impact
Long-Term Management and Follow-Up
Regular outpatient cardiology follow-up is recommended to monitor for disease progression and optimize medical therapy.
📅 Follow-Up Recommendations
- Cardiology follow-up within 2-4 weeks
- Consider ambulatory monitoring (Holter or event recorder) for symptom correlation
- Lifestyle modifications: regular exercise, stress reduction, adequate sleep, avoid triggers (caffeine, alcohol, stimulants)
- Patient education on warning symptoms requiring immediate medical attention
Common Pitfalls and How to Avoid Them
⚠️ Critical Mistakes to Avoid
- Misdiagnosis risk: Always compare to prior ECGs when available - new findings are more significant than chronic changes
- Treatment errors: Avoid treating the ECG in isolation - clinical context and hemodynamic status determine urgency
- Delayed recognition: Unstable patients require immediate intervention, not prolonged workup
- Medication errors: Check medication interactions and contraindications before administration
- Disposition errors: Ensure appropriate level of care and monitoring based on risk stratification
Patient Education and Shared Decision-Making
When counseling patients diagnosed with Right Bundle Branch Block (RBBB), address these important topics:
- Diagnosis explanation: Use simple language avoiding medical jargon - "Your heart's electrical system shows..." rather than complex terminology
- Prognosis discussion: Provide realistic expectations about symptom control, treatment success rates, and quality of life
- Warning signs: Teach patients to recognize symptoms requiring immediate emergency care (chest pain, severe shortness of breath, syncope, palpitations with dizziness)
- Medication adherence: Importance of taking medications as prescribed, managing side effects
- Lifestyle modifications: Limit caffeine and alcohol, maintain healthy weight through diet and exercise, stress management techniques, adequate sleep hygiene
- Activity guidance: Generally no restrictions once symptoms controlled and rhythm stable
- Family screening: Discuss cardiovascular risk factors with family members
Evidence-Based Guidelines and Key Trials
Current management of Right Bundle Branch Block (RBBB) is based on high-quality evidence from landmark clinical trials and consensus guidelines from major professional societies:
- American Heart Association (AHA) / American College of Cardiology (ACC) - Comprehensive guidelines for cardiac rhythm management
- European Society of Cardiology (ESC) - Evidence-based recommendations for arrhythmia management
- Advanced Cardiac Life Support (ACLS) - Standardized protocols for emergency cardiac care
- Heart Rhythm Society (HRS) - Expert consensus statements on electrophysiology and device therapy
📚 Level of Evidence
Recommendations for management of Right Bundle Branch Block (RBBB) are primarily supported by Level B evidence (limited randomized trials, high-quality observational studies, and registry data).
Summary and Clinical Bottom Line
📋 Clinical Bottom Line
Right Bundle Branch Block (RBBB) is characterized by qrs >120ms (wide) on ECG. May be normal variant or indicate RV strain/pathology, ischemia still interpretable unlike LBBB Primary management: Investigate for underlying cause if new, evaluate for pulmonary embolism if acute onset, usually no specific treatment Key takeaway: Prompt diagnosis and evidence-based therapy optimize patient outcomes and prevent complications
About the Author
Dr. Raj K
Emergency Medicine Physician Dr. Raj K is a board-certified Emergency Medicine physician with extensive experience in acute cardiac emergencies, advanced ECG interpretation, and critical care. He is passionate about medical education and bringing evidence-based emergency medicine knowledge to healthcare providers worldwide through E-PulsePoints. His clinical expertise includes STEMI management, complex arrhythmia recognition, and emergency cardiac procedures.